
 Mon - Sun 8:00 - 19:00
Mon - Sun 8:00 - 19:00Dental implants represent a highly predictable restorative solution in modern dentistry, but they are not entirely immune to biological or mechanical complications. When patients ask about dental implant failure symptoms, the clinical signs are generally categorized into distinct early and late stages. Early warnings primarily involve peri-implant mucositis, which manifests as red, swollen, or tender mucosal tissues surrounding the titanium post, often accompanied by bleeding during routine brushing. As the pathological condition progresses into active infection, the symptoms become significantly more severe and destructive. Patients will typically experience spontaneous suppuration or pus discharge, persistent halitosis, a dull metallic taste, radiating discomfort, and visible mucosal recession exposing the underlying metal threads. In the final terminal phase of failure, the artificial tooth root loses its rigid integration with the surrounding jawbone, resulting in noticeable mechanical mobility. Identifying these clinical warning signs rapidly allows dental specialists to intervene with non-surgical or targeted debridement therapies, halting the osseous destruction before complete fixture extraction becomes the absolute only viable medical option.
The statistical prevalence of biological complications demands rigorous clinical monitoring for all implant recipients. The International Team for Implantology (ITI) consensus reports that 24.1% of bleeding-on-probing (BOP) positive implants will eventually be diagnosed with destructive peri-implantitis. Furthermore, longitudinal epidemiological data presented at the World Workshop on Periodontology indicates that progressive peri-implant bone loss exceeding 2 millimeters occurs in 20.1% of clinical cases after five years of functional loading. Smoking exponentially elevates these risks, yielding a staggering 36.3% disease occurrence rate among tobacco users.
Recognizing Early vs. Late Dental Implant Failure Symptoms
Recognizing the exact phase of biological complication dictates the required medical intervention. Early failure symptoms include localized mucosal bleeding, swelling, and tenderness without any underlying bone destruction, defining a reversible condition called mucositis. Late failure symptoms involve irreversible alveolar bone loss, persistent purulent discharge, deep periodontal pocketing, and ultimate fixture mobility, clinically diagnosed as peri-implantitis. Immediate identification dictates the survival of the restoration.
The clinical success of an osseointegrated fixture relies entirely on the structural integrity of the surrounding biological envelope. Unlike natural dentition, which is suspended within the alveolar bone by a highly vascularized periodontal ligament, a Titanium implant relies on direct, rigid bone-to-implant contact (BIC). This fundamental anatomical difference means that implants lack the robust localized immune defense mechanisms provided by the periodontal ligament’s blood supply. Consequently, when the soft tissue seal around the abutment is breached by bacterial pathogens, the ensuing inflammatory cascade can rapidly precipitate implant failure. Recognizing early dental implant failure symptoms is critical for saving the artificial tooth root before the supporting jawbone undergoes irreversible necrosis and resorption.
The symptomatology of implant failure exists on a clinical spectrum. In the preliminary phase, clinically defined as peri-implant mucositis, the inflammatory lesion is strictly confined to the mucosal soft tissues. Patients will visually observe localized erythema (redness) and edema (swelling) at the gingival margin. The hallmark diagnostic sign at this stage is bleeding upon minimal mechanical provocation, such as gentle domestic flossing or professional clinical probing. Importantly, this phase is characterized by the complete absence of marginal bone loss. Because the osseous architecture remains intact, mucositis is entirely reversible through targeted mechanical debridement and strict optimization of the patient’s daily oral hygiene regimen.
Conversely, if mucositis is left untreated, the dysbiotic biofilm advances apically, initiating the devastating phase known as peri-implantitis. This condition is characterized by a hyper-responsive host immune reaction that inadvertently activates osteoclastic cells—the cells responsible for breaking down bone tissue. The clinical presentation of late-stage failure is highly distressing. Patients frequently report spontaneous suppuration (the active exudation of yellowish pus from the peri-implant sulcus), accompanied by chronic halitosis and a foul, metallic taste that persists despite aggressive mouthwashing. The gingival tissues often undergo severe recession, exposing the micro-roughened threads of the Titanium fixture to the oral cavity, which accelerates plaque accumulation. Pain is relatively uncommon in the early stages but manifests as a dull, throbbing ache radiating through the jawbone once the infection reaches the apical region. The absolute terminal symptom of this pathological progression is clinical mobility. An integrated implant should remain rigidly fixed; any detectable movement under occlusal pressure confirms the catastrophic loss of osseointegration, mandating immediate surgical explantation.
The visual representation below clarifies how bacterial colonies infiltrate the sulcular space, initiating the localized destruction of critical osseous structures.
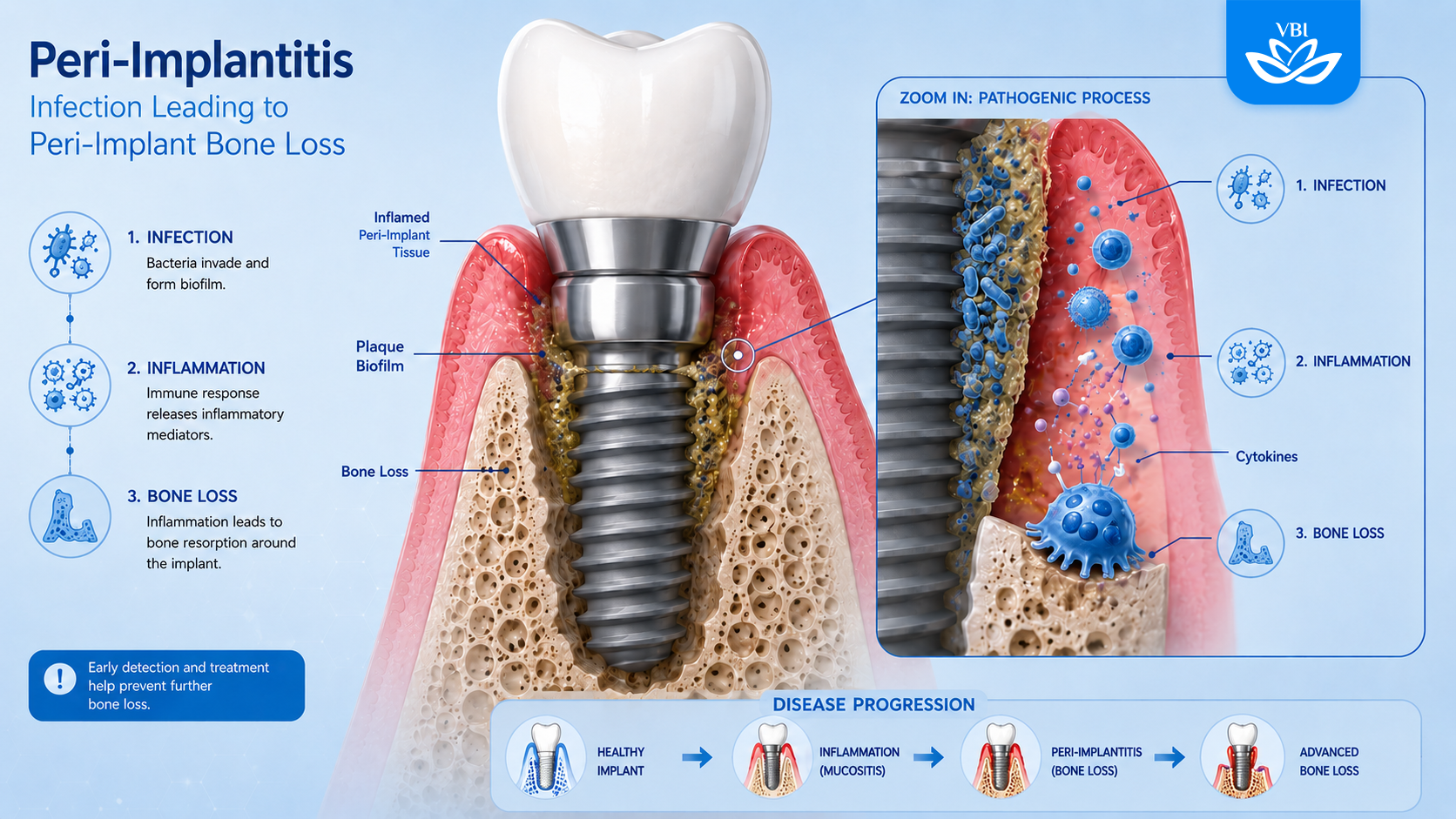
The Biological Pathogenesis of Peri-Implantitis
The transition from localized tissue inflammation to aggressive bone destruction is driven by a complex microbiological cascade. Pathogenic biofilms colonize the micro-roughened titanium surface, triggering a hyper-responsive host immune reaction. This chronic inflammatory infiltrate subsequently activates osteoclastic cells, which resorb the supporting jawbone. Without intervention, this infectious pathway severs the critical osseointegration interface, permanently destabilizing the entire prosthetic rehabilitation architecture.
To fully comprehend the destructive nature of these complications, one must examine the microbiological environment of the oral cavity. Within hours of surgical placement, the Titanium surface is coated by a salivary pellicle, providing an adhesive substrate for primary bacterial colonizers. In a healthy state, this biofilm is continuously disrupted by mechanical brushing. However, when oral hygiene is compromised, the biofilm matures, shifting from a predominantly aerobic, Gram-positive flora to a highly pathogenic, Gram-negative anaerobic bacterial complex. These virulent microorganisms, including Porphyromonas gingivalis and Treponema denticola, thrive in the oxygen-deprived environment of the peri-implant sulcus.
As these pathogens multiply, they release potent endotoxins and tissue-degrading enzymes. The human immune system responds by deploying macrophages and neutrophils to the site of infection. While these defensive cells attempt to neutralize the bacteria, they simultaneously release pro-inflammatory cytokines (such as Interleukin-1$\beta$ and Tumor Necrosis Factor-$\alpha$). In the unique microenvironment of the jawbone, high concentrations of these cytokines disrupt the delicate balance between bone formation (osteoblasts) and bone resorption (osteoclasts). The resulting cytokine storm hyper-activates the osteoclasts, leading to the rapid, crater-like destruction of the alveolar bone surrounding the implant fixture.
The topography of the implant itself plays a paradoxical role in this disease model. Modern fixtures are engineered with micro-roughened surfaces (such as Sandblasted, Large-grit, Acid-etched surfaces) specifically designed to accelerate initial bone healing and maximize cellular adhesion. However, if marginal bone loss occurs and these highly porous threads become exposed to the oral cavity, they act as an ideal, highly retentive harbor for plaque accumulation. Decontaminating a rough Titanium surface once it has been colonized by an established biofilm is exceptionally difficult, rendering non-surgical interventions largely ineffective once deep pocketing has occurred.
Intrinsic and Extrinsic Etiological Risk Factors
Implant stability relies heavily on patient physiology and precise biomechanical engineering. Intrinsic risks include poorly controlled diabetes mellitus and a prior history of aggressive periodontitis, which fundamentally compromise immune responses. Extrinsic factors involve tobacco consumption, which restricts capillary blood flow, alongside iatrogenic surgical errors such as retained dental cement, inadequate restorative emergence profiles, and occlusal overload on the prosthetic framework.
The etiology of implant failure is distinctly multifactorial. Clinical epidemiological studies have conclusively isolated several high-risk profiles that predispose patients to biological complications. The most critical intrinsic risk factor is a documented history of severe periodontitis. Patients who have lost their natural dentition to aggressive gum disease harbor a highly virulent oral microbiome. These periodontal pathogens easily translocate from the remaining natural teeth or the mucosal reservoirs to the newly placed sterile implants, initiating the peri-implantitis cascade at an accelerated rate.
Systemic medical conditions, particularly diabetes mellitus, exert a profound negative influence on osseointegration. Chronic hyperglycemia impairs neutrophil function, diminishing the body’s ability to combat localized infections. Furthermore, elevated blood glucose levels interfere with collagen synthesis and capillary proliferation, fundamentally disrupting the bone healing process. Patients with an HbA1c level exceeding 8.0% face an exponentially higher risk of both early surgical failure and late-stage peri-implantitis.
Extrinsic behavioral factors are equally destructive. Tobacco smoking remains the most significant controllable risk factor in implant dentistry. The nicotine and carbon monoxide absorbed during smoking induce severe peripheral vasoconstriction, drastically reducing the microcirculation of oxygenated blood to the peri-implant tissues. This hypoxic environment not only suppresses the immune response but also inhibits the proliferation of osteoblasts, making heavy smokers highly susceptible to catastrophic bone loss. If a patient experiences severe pain or swelling, understanding precisely what to do if implant fails requires immediate cessation of tobacco use alongside emergency clinical intervention.
Beyond biological factors, iatrogenic (clinician-induced) variables frequently act as the catalyst for failure. The restorative phase carries significant risks if not executed with millimeter precision. One of the leading causes of acute, rapid-onset peri-implantitis is the incomplete removal of excess dental cement. When a porcelain crown is cemented onto the implant abutment, microscopic fragments of the luting agent can easily be forced deep into the subgingival sulcus. Because the peri-implant tissues cannot biologically attach to acrylic or resin-modified glass ionomer cements, these retained fragments act as a highly irritating foreign body, providing an unyielding scaffold for pathogenic bacterial colonization. Furthermore, biomechanical overload resulting from improper occlusal calibration, heavy bruxism (teeth grinding), or poorly designed restorative emergence profiles can induce micro-fractures in the crestal bone, initiating aseptic (non-infectious) bone resorption that mimics the symptoms of bacterial peri-implantitis.
Diagnostic Protocols and Clinical Assessments
Accurate diagnosis demands a dual approach utilizing both tactile clinical examination and advanced radiographic imaging. Dental specialists perform gentle peri-implant probing to assess pocket depth variations and identify signs of suppuration or bleeding. Simultaneously, high-resolution cone-beam computed tomography (CBCT) or periapical radiographs are utilized to quantify crestal bone stability, differentiating natural physiological remodeling from aggressive, infection-driven pathological bone loss.
The definitive diagnosis of biological complications requires extreme precision, as the clinical presentation of physiological bone remodeling can occasionally mimic active infection. According to the foundational consensus reports, the cornerstone of diagnostic monitoring is the standardized periodontal probe. Clinicians must meticulously measure the probing depth (PD) around the entire circumference of the restoration. To prevent iatrogenic damage to the fragile mucosal seal, this probing must be executed with a strictly calibrated, light force of 0.2 to 0.25 Newtons.
Under baseline healthy conditions, probing depths around a conventionally placed fixture generally range from 2 to 4 millimeters. Any longitudinal increase beyond these baseline measurements, accompanied by Bleeding on Probing (BOP), serves as the primary diagnostic indicator of an active inflammatory lesion. The presence of suppuration upon digital palpation of the marginal gingiva further confirms a highly active, purulent infection requiring immediate interception.
However, clinical parameters alone are insufficient to confirm a diagnosis of peri-implantitis; radiographic evidence of crestal bone destruction is the absolute diagnostic prerequisite. Establishing an accurate baseline is critical. Following the surgical installation of the prosthetic abutment and the application of functional occlusal loading, a degree of initial crestal bone remodeling (typically up to 1-1.5 millimeters) is physiologically normal and expected. True peri-implantitis is defined by progressive, saucer-shaped bone loss that extends beyond this initial remodeling phase. In scenarios where historical baseline radiographs are unavailable for direct comparison, international clinical guidelines mandate that a threshold of 2 millimeters of crestal bone loss, combined with clinical signs of inflammation, must be met to confirm the diagnosis. To understand the exhaustive criteria utilized by global specialists, patients and practitioners can review the clinical peri-implantitis guidelines established by leading academic consortiums.
Modern dental clinics utilize highly specialized optical equipment to vaporize embedded pathogens without damaging the delicate titanium micro-threads.

Comprehensive Surgical and Non-Surgical Treatment Protocols
Arresting the progression of implant disease requires specific, targeted decontamination of the titanium surface. Non-surgical therapies utilize ultrasonic scaling and antimicrobial irrigation for localized mucositis. However, advanced bone loss necessitates surgical flap reflection to directly access the infected root. Regenerative procedures involving specialized bone grafting materials are then applied to reconstruct the lost osseous architecture and restabilize the failing fixture.
The therapeutic management of peri-implant diseases represents one of the most formidable challenges in contemporary restorative dentistry. The primary objective of all intervention protocols is the complete eradication of the pathogenic biofilm, the resolution of soft tissue inflammation, and the arrest of progressive osteoclastic bone destruction. The specific treatment modality deployed is entirely dependent on the severity of the defect, emphasizing why recognizing early dental implant failure symptoms is absolutely paramount.
For patients diagnosed exclusively with peri-implant mucositis, non-surgical mechanical therapy is highly effective. This protocol involves the meticulous debridement of the prosthetic components utilizing specialized Carbon-fiber or Titanium curettes, which are specifically designed to remove calcified plaque deposits without scratching the machined surface of the abutment. Ultrasonic scaling devices equipped with polymeric tips are utilized in conjunction with continuous antimicrobial irrigation (such as 0.12% Chlorhexidine Gluconate or Povidone-Iodine solutions). Additionally, air-polishing systems utilizing low-abrasive Glycine or Erythritol powders have demonstrated exceptional efficacy in disrupting submucosal biofilms while preserving the integrity of the soft tissue attachment.
However, once the pathology crosses the threshold into destructive peri-implantitis, non-surgical interventions are universally considered inadequate. The deep, crater-like bony defects restrict the physical access of standard scaling instruments, making it biologically impossible to decontaminate the rough, porous threads of the Titanium fixture blindly. In these advanced scenarios, full-thickness mucoperiosteal flap surgery is mandatory. The oral surgeon must reflect the gingival tissues to achieve direct visual access to the contaminated site. Granulation tissue is meticulously excised, and the exposed Titanium surface undergoes rigorous physical and chemical decontamination. Effective peri implantitis treatment involves advanced laser decontamination and professional cleaning. Specifically, the utilization of Erbium-doped Yttrium Aluminum Garnet (Er:YAG) lasers or photodynamic therapy (PDT) has revolutionized the decontamination phase, as these technologies possess the unique ability to vaporize bacterial endotoxins embedded deep within the titanium micro-pores without inducing thermal damage to the adjacent vital bone.
Following surface detoxification, the surgeon must address the osseous defect. Depending on the morphology of the bone loss (e.g., narrow three-wall defects versus wide circumferential defects), regenerative therapy may be attempted. This involves packing the decontaminated site with particulate bone graft materials (Xenografts or Alloplasts) and sealing the area with a resorbable collagen membrane to facilitate the regeneration of native bone and attempt re-osseointegration. If the defect architecture is not conducive to regeneration, resective surgery (implantoplasty) is performed. This involves utilizing high-speed diamond burs to mechanically obliterate the exposed micro-threads, creating a perfectly smooth, polished Titanium surface that prevents future plaque retention, followed by the apical repositioning of the mucosal tissues.
Preventive Maintenance and International Warranty Assurance
The long-term success of an implant rehabilitation strictly depends on consistent, professional maintenance protocols. Patients must adhere to biannual clinical assessments and rigorous domestic hygiene routines to prevent biofilm accumulation. For those engaging in cross-border dental tourism, securing an international warranty ensures that any unforeseen biological complications are managed swiftly, protecting the substantial financial and physiological investment made abroad.
The biological reality of osseointegrated prosthetics dictates that patient responsibility does not end on the day the final ceramic crown is seated. Implants require a higher standard of hygiene maintenance than natural dentition. Patients must utilize specifically designed interdental brushes, low-abrasive dentifrices, and oral irrigators (water flossers) to aggressively disrupt plaque accumulation at the vulnerable restorative margins. Professional clinical assessments, including radiographic screening and prophylactic scaling, must be scheduled at strict 4-to-6-month intervals to intercept mucositis before it cascades into irreversible bone loss.
For the rapidly expanding demographic of international patients participating in dental tourism—traveling from high-cost regions like Australia, the United States, or the United Kingdom to premium clinical hubs in Vietnam—managing complications requires a formalized logistical framework. Reputable international clinics mitigate the anxieties associated with cross-border healthcare by offering transparent, legally binding global warranties on both the Titanium fixtures and the Zirconia suprastructures.
Understanding your rights and clinical safety nets is vital. Patients undergoing complex full-arch rehabilitations (such as All-on-4 or All-on-6 protocols) must ensure their chosen clinic provides clear, asynchronous communication channels for post-surgical triage. If you experience swelling, bleeding, or structural issues upon returning to your home country, immediate remote consultation enables the original surgical team to dictate the correct emergency protocol. To comprehensively understand how advanced clinical networks protect your investment across international borders, review the details regarding global warranty coverage provided by certified facilities.
Contact our emergency dental specialists via WhatsApp for an immediate consultation regarding your post-surgical symptoms and targeted medical rescue protocols.



Bài viết liên quan
Porcelain Veneers vs. Crowns: Enamel Preservation Comparison
When choosing between treatments, understanding the veneers vs crowns enamel preservation trade-off is vital for...
Sensitive Teeth After Laser Whitening: What to Do (Expat Guide)
Medical Disclaimer: This information is for educational purposes only and does not constitute medical advice....
Why Do My Gums Bleed When Brushing? Causes & Solutions for Expats
(Disclaimer: This content is for educational purposes only and does not replace professional dental advice.)...
Do Dental Implants Hurt? Pain Management in Vietnam Clinics
Many patients ask whether the procedure will cause significant discomfort. The definitive clinical reality is...
The Hidden Risks of Cheap Dental Implants Overseas
Seeking affordable dental care abroad sounds highly appealing. But what are the actual cheap dental...
Using Super for Dental Implants: Australian Guidelines 2026
Many patients ask about using super for dental implants and navigating the ATO compassionate release...