
 Mon - Sun 8:00 - 19:00
Mon - Sun 8:00 - 19:00The deterioration of alveolar bone tissue begins immediately following tooth extraction. This rapid physiological decline presents a severe structural challenge for restorative dentistry. Without the mechanical load of chewing, the jawbone undergoes aggressive resorption, losing vertical height and horizontal width. A bone graft for dental implants effectively halts this degradation. The procedure introduces a specialized osteoconductive matrix into the deficient anatomical site. This matrix prompts your biological system to regenerate lost cellular density. Clinical data unequivocally demonstrates that successful osseointegration demands a pristine, dense skeletal foundation. Advanced methodologies, particularly utilizing ultrasonic piezoelectric instrumentation, have dramatically transformed the surgical experience. The intervention is precise. Tissue trauma is minimal. For individuals exploring permanent rehabilitation, understanding when you need a bone graft for dental implants is crucial for long-term stability and functional restoration.
The Anatomy of the Alveolar Process and Mechanical Loading
The structural integrity of the human maxillofacial skeleton relies heavily on a complex biomechanical feedback loop. The alveolar process, the thickened ridge of bone that contains the tooth sockets, is a highly dynamic structure. It is not a static anatomical entity but rather a living, constantly remodeling tissue matrix. Its primary physiological function is to anchor the roots of the natural dentition and to absorb, distribute, and dissipate the immense occlusal forces generated during mastication.
When a patient chews, mechanical stress is transmitted through the crown of the tooth, down the root, and into the surrounding periodontal ligament. This ligament acts as a biological shock absorber, converting mechanical pressure into tension on the surrounding alveolar bone. According to Wolff’s Law of bone transformation, bone in a healthy person or animal will adapt to the loads under which it is placed. If loading on a particular bone increases, the bone will remodel itself over time to become stronger to resist that sort of loading. The inverse is equally true and clinically significant: if the mechanical loading decreases or ceases entirely, the bone will become less dense and weaker due to the lack of the stimulus required for continued remodeling.
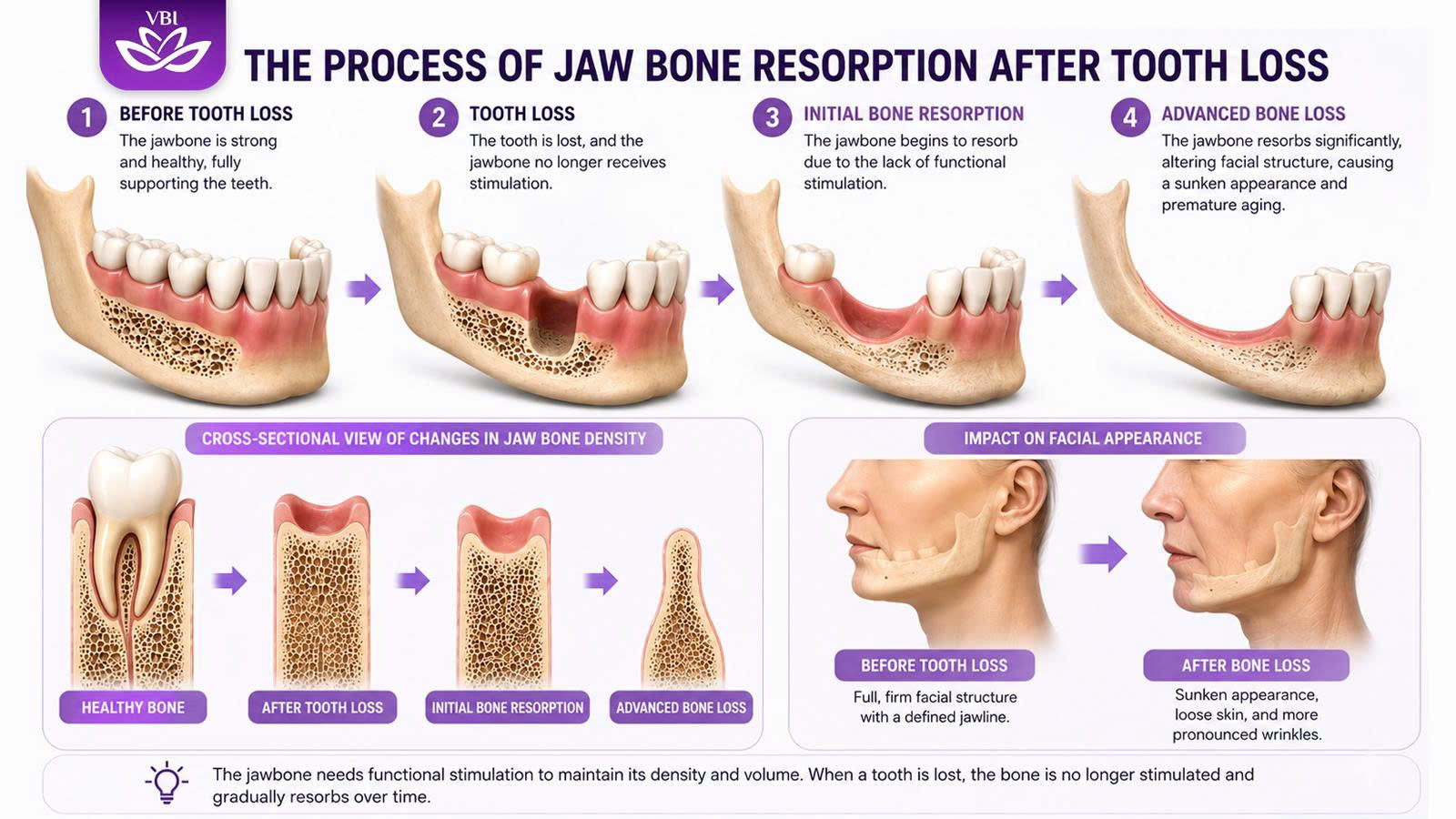
This biomechanical principle explains why tooth loss is catastrophically detrimental to jaw structure. The extraction of a tooth removes the occlusal load entirely. The periodontal ligament is severed, and the localized tension on the alveolar bone drops to zero. The body, functioning as an incredibly efficient biological machine, interprets this lack of mechanical stimulation as a signal that the bone in that specific area is no longer structurally necessary. Consequently, the physiological process of bone maintenance is halted, and the body initiates a localized mechanism to reclaim the calcium and minerals from the redundant bone matrix, distributing them to other areas of the body where they might be needed. This process results in a rapid and progressive loss of both alveolar bone volume and density, setting the stage for significant restorative complications.
The Pathophysiology of the Bone Resorption Process
To comprehend the necessity of regenerative surgery, one must analyze the biochemical cascade that drives tissue degradation. The physiological response to tooth loss is immediate. The alveolar bone begins to atrophy through a cellular mechanism known universally as bone resorption. While bone resorption is a basic, necessary physiologic process central to overall skeletal maintenance and calcium homeostasis, it becomes a pathological localized event following dental extractions.
At the histological level, bone remodeling is dictated by the delicate, continuous balance between two primary cell types: osteoblasts, the cells responsible for synthesizing and mineralizing the bone matrix, and osteoclasts, the highly specialized, multinucleated cells responsible for the dissolution and absorption of bone. Following the loss of a tooth, the localized trauma and the abrupt cessation of occlusal loading trigger a profound disruption in this cellular equilibrium. The activity of osteoclasts accelerates drastically, outpacing the regenerative efforts of the osteoblasts.
In the oral environment, specific signaling proteins called cytokines critically influence this balance between tissue resorption and regeneration. Cytokines act as molecular messengers, regulating inflammatory pathways and cellular behavior. The surgical trauma of an extraction induces a localized inflammatory microenvironment. Within this environment, cytokines orchestrate a cascade that heavily favors tissue destruction. They stimulate the differentiation and activation of osteoclast-like cells, which then attach to the bone surface and secrete highly acidic compounds and proteolytic enzymes. These secretions dissolve the inorganic hydroxyapatite crystals and degrade the organic collagen matrix of the bone.
This cytokine-driven tissue destruction is highly specific and biochemically measurable. Clinical assessments and laboratory analyses can often identify the presence of specific biomarkers, such as Pyridinoline cross-links. These cross-links are molecular structures that stabilize collagen in bone and cartilage. Their release into the bloodstream and subsequent excretion are highly specific indicators of active bone resorption. Furthermore, pathological root resorption (PRR) represents a clinically significant model of this cytokine-driven tissue destruction, where the inflammatory microenvironment leads to the breakdown of dental hard tissues. Understanding these shared molecular pathways underscores why halting the resorptive process requires immediate and precise surgical intervention.
If this aggressive resorptive process is left unchecked by restorative measures, the alveolar ridge loses its vertical dimension and its horizontal width, culminating in a knife-edge ridge that cannot support a titanium root.
Before implementing any specific regenerative protocol, advanced digital diagnostics must accurately map the extent of this cellular degradation.
Biomaterial Science: The Triad of Bone Regeneration
The central objective of any augmentation procedure is to provide a stable, three-dimensional scaffold capable of inducing cell migration and tissue in-growth at the material interface. The success of this endeavor depends entirely on the biological and mechanical properties of the chosen grafting material. In modern biomaterial science, an ideal grafting matrix is evaluated based on its capacity to fulfill three distinct regenerative mechanisms: osteogenesis, osteoinduction, and osteoconduction.
Osteogenesis refers to the direct formation of new bone by living cells contained within the graft material itself. This requires the presence of viable, surviving osteoblasts and osteoprogenitor cells that can actively synthesize new bone matrix immediately upon transplantation.
Osteoinduction is a biochemical process whereby the graft material actively stimulates the host’s undifferentiated mesenchymal stem cells to differentiate into bone-forming osteoblasts. This is typically mediated by specific growth factors, most notably Bone Morphogenetic Proteins (BMPs), which are naturally present in the bone matrix and are released during the remodeling process. An osteoinductive graft acts as a biological catalyst, actively recruiting the body’s healing mechanisms to the surgical site.
Osteoconduction is a physical phenomenon. It refers to the ability of the graft material to serve as an inert, three-dimensional scaffold or framework upon which the host’s native osteoblasts and newly formed blood vessels can migrate, attach, and proliferate. An osteoconductive material does not actively stimulate bone growth or provide living cells; it simply provides the structural roadmap for the body’s natural regenerative processes to follow. The efficacy of an osteoconductive scaffold is heavily dependent on its macroscopic and microscopic porosity, which must mimic the natural trabecular architecture of human bone to facilitate cellular infiltration and angiogenesis.
Autologous Grafts: The Biological Gold Standard
In the hierarchy of grafting materials, autologous bone—bone harvested directly from the patient’s own body—remains the definitive gold standard against which all other substitutes are measured. Autografts are the only materials that natively possess the complete triad of regenerative properties: they are simultaneously osteogenic, osteoinductive, and osteoconductive.
The harvesting of autogenous bone is typically performed at intraoral sites, such as the mandibular ramus (the vertical part of the lower jaw), the mandibular symphysis (the chin), or the maxillary tuberosity. For larger maxillofacial defects requiring massive reconstructive efforts, extraoral donor sites like the anterior or posterior iliac crest (the hip bone) or the calvarium (the skull) may be utilized.
When an autograft is transferred to the recipient site, the surviving osteoblasts within the graft immediately begin synthesizing new bone matrix (osteogenesis). Simultaneously, the organic matrix of the transplanted bone releases potent growth factors, including various BMPs, which actively recruit and differentiate host stem cells (osteoinduction). Finally, the mineralized structure of the autograft provides the perfect, biologically identical scaffold for the newly forming tissue (osteoconduction). This comprehensive biological activity results in the fastest integration time, the highest quality of newly formed bone, and the lowest theoretical risk of immune rejection, as the material is entirely biologically compatible with the host.
However, despite these unparalleled biological advantages, autografts present significant and often prohibitive clinical drawbacks. The primary limitation is the absolute necessity of a second surgical site to harvest the material. This significantly increases donor-site morbidity, prolongs the overall duration of the surgical intervention, and exposes the patient to additional postoperative pain, swelling, and potential complications at the harvest location. Furthermore, there is a distinctly limited availability of harvestable intraoral bone. A patient’s mandibular symphysis or ramus can only yield a small volume of grafting material, rendering intraoral autografts unsuitable for extensive ridge augmentations or bilateral sinus elevations. Lastly, freshly harvested autologous bone exhibits a rapid resorption rate in vivo. Because it is highly cellular and biologically active, the body’s osteoclasts begin remodeling it immediately. Consequently, a significant portion of the grafted volume may be resorbed before complete structural stabilization occurs, requiring the surgeon to over-graft the site to compensate for this anticipated loss.
Allogeneic Grafts: Human-Derived Matrices
To circumvent the morbidity and volume limitations associated with autogenous harvesting, allografts serve as a highly effective and frequently utilized alternative. Allografts are derived from genetically non-identical human donors, typically sourced from certified tissue banks following the processing of cadaveric bone.
The utilization of human donor tissue requires rigorous screening, extensive processing, and terminal sterilization protocols to ensure absolute safety and to eliminate any theoretical risk of disease transmission or severe immunological rejection. This intensive processing inevitably strips the material of all living cellular components, meaning allografts lack the osteogenic capacity of autografts. However, the specific processing methods dictate the remaining biological properties of the material.
Allografts are generally available in two primary forms: Mineralized Freeze-Dried Bone Allografts (FDBA) and Demineralized Freeze-Dried Bone Allografts (DFDBA). FDBA provides excellent structural support and acts primarily as a slow-resorbing osteoconductive scaffold. Conversely, the demineralization process used to create DFDBA removes the inorganic mineral phase of the bone, exposing the underlying organic collagen matrix and, crucially, the trapped Bone Morphogenetic Proteins (BMPs). Consequently, while DFDBA lacks mechanical rigidity, it retains significant osteoinductive capabilities. The exposed BMPs are capable of actively stimulating the host’s mesenchymal stem cells to differentiate into osteoblasts, promoting robust ectopic bone formation.
By eliminating the need for a secondary harvest surgery, allografts significantly improve patient comfort and reduce surgical time while offering an effectively infinite supply of grafting volume. They remain a staple in periodontal regeneration and localized ridge augmentations.
Xenogeneic Grafts: The Bovine Bone Superiority
Xenografts represent a highly sophisticated category of grafting materials derived from a genetically unrelated species. In the modern dental field, the most common and clinically documented source of xenograft material is deproteinized bovine bone, commercially recognized under brand names such as BioOss, OsteoGraf, and Cerabone.
The manufacturing process of bovine xenografts is an marvel of biomaterial engineering. To render the animal bone safe for human implantation and to completely eliminate the risk of zoonotic disease transmission or immune rejection, the raw bovine bone is subjected to a rigorous, stepwise annealing process. This involves extreme high-temperature treatment combined with harsh chemical processing, typically utilizing strong alkalis like Sodium Hydroxide (NaOH). This extreme purification eradicates all organic components, proteins, and cellular debris, leaving behind only the pure, inorganic mineral phase of the bone.
The resulting product is a highly porous hydroxyapatite material that exhibits exceedingly low immunogenicity. Crucially, the macroscopic and microscopic structural architecture of this purified bovine mineral is virtually identical to human cancellous (spongy) bone. The mechanical properties of xenografts are exceptional for specific clinical applications. While they are strictly osteoconductive and lack any innate osteoinductive or osteogenic properties , their vast surface area and interconnected porous network promote robust angiogenesis. The ingrowth of new blood vessels is the fundamental prerequisite for bone healing, as it delivers the necessary oxygen, nutrients, and osteoprogenitor cells to the core of the graft.
The clinical efficacy of bovine xenografts in large-volume augmentations is undeniable. Histological studies have demonstrated that maxillary defect sites augmented exclusively with bovine xenografts resulted in 39% new vital bone formation after a six-month healing period. This figure is remarkably comparable to the 40% new bone formation observed following grafting with autologous bone under identical conditions.
Where xenografts truly excel, however, is in their volumetric stability. Because the high-temperature processing alters the crystalline structure of the hydroxyapatite, xenografts are highly resistant to rapid osteoclastic resorption. Research indicates that 31% of the grafted bovine material remained structurally intact at the surgical site after six months, acting as a permanent, stabilizing matrix, compared to only 18% retention of autograft bone. This slow resorption profile makes xenografts the material of absolute choice for procedures where long-term space maintenance is critical, such as sinus floor elevations and the repair of large cystic cavities.
Specialized surgical preparation ensures that the integration of these animal-derived matrices yields highly predictable clinical outcomes.

Alloplastic Synthetic Scaffolds and Ectopic Bone Formation
Alloplastic materials are entirely synthetic grafts engineered meticulously in laboratory settings, representing the frontier of biomaterial science. These include various calcium-phosphate-based ceramics, such as synthetic hydroxyapatite (HA), beta-tricalcium phosphate (β-TCP), biphasic calcium phosphate (BCP), and advanced bioactive glasses. The primary overarching advantage of alloplasts is their infinite commercial availability, consistent batch-to-batch quality, and the absolute elimination of any biological risks regarding disease transmission or ethical concerns associated with human or animal donors.
Historically, synthetic grafts were regarded purely as inert, osteoconductive space maintainers. They provided a physical matrix but relied entirely on the host’s native biology to initiate the healing cascade. They often suffered from limitations such as medium mechanical strength with a high probability of fragility, and very slow degradability that sometimes required resurgery if the material failed to integrate.
However, recent revolutionary advancements in biomaterial engineering have fundamentally altered the clinical capabilities of synthetic grafts. The development of novel Biphasic Calcium Phosphate (BCP) scaffolds has shown unprecedented results. BCP is a precise mixture of stable hydroxyapatite and rapidly resorbable beta-tricalcium phosphate. When fabricated and sintered at specific low temperatures, these novel BCP scaffolds exhibit unique surface micro-topographies and dissolution profiles.
Remarkably, clinical and in vivo studies have demonstrated that these advanced, low-temperature sintered BCP synthetic bone grafts possess the ability to induce ectopic bone formation in non-skeletal sites without the exogenous addition of osteoinductive growth factors like BMP-2. This means the synthetic material itself can trigger osteoinduction based purely on its physiochemical properties and its high strength of interaction with cells via chemical bonds. The complete similarity of their structures to native minerals ensures high biocompatibility, high potential for osseointegration, and a structural similarity to bone tissue in terms of components and cavities. These studies demonstrate that newly developed synthetic bone grafts have the potential for inducing bone formation similar to highly processed biological allografts like DFDBA.
In the near future, alloplastic bone substitutes with standardized quality and engineered safety profiles may become the primary choice over autologous bone, offering new osteoconductive and osteoinductive products with optimal handling forms and controlled resorption rates.
| Graft Category | Source Material | Primary Biological Properties | Key Clinical Advantages | Inherent Limitations |
| Autograft | Patient’s own skeletal sites | Osteogenic, Osteoinductive, Osteoconductive | Absolute biocompatibility, fastest cellular integration. |
Second surgical site, high donor morbidity, rapid resorption. |
| Allograft | Human cadaveric tissue | Osteoinductive (DFDBA), Osteoconductive | Eliminates donor morbidity, wide availability. |
Lacks living osteoblasts, intensive processing required. |
| Xenograft | Deproteinized Bovine bone | Highly Osteoconductive |
Exceptional volume stability, high porosity for robust angiogenesis. |
Very slow resorption, natively lacks osteoinduction. |
| Alloplast | Synthetic Ceramics (BCP) | Osteoconductive, potentially Osteoinductive |
Infinite supply, zero disease transmission, highly engineered micro-topography. |
Can be brittle, lacks organic phase for cellular remodeling. |
The Maxillary Sinus Challenge and Subantral Augmentation
While grafting extraction sockets or narrow ridges in the mandible presents specific challenges, the posterior maxilla—the upper jaw region previously occupied by molars and premolars—presents arguably the most complex anatomical environment for restorative implantology.
Following the extraction of maxillary posterior teeth, the alveolar bone resorbs vertically upwards toward the base of the skull. Simultaneously, a unique anatomical phenomenon occurs: the maxillary sinus cavity, large air-filled spaces situated directly above the roots of the upper teeth, tends to pneumatize. Pneumatization is the biological process where the air cavity expands downwards and laterally into the space once occupied by the dental roots and the supporting alveolar bone. The resulting dual-action bone loss—resorption from below and pneumatization from above—often leaves a paper-thin layer of cortical bone separating the oral cavity from the sinus. This remaining bone volume is entirely insufficient to anchor a titanium fixture safely. Attempting to place an implant in this compromised anatomy would result in the fixture protruding directly into the sinus cavity, leading to severe chronic sinusitis, graft failure, and the loss of the implant.
To overcome this severe anatomical limitation, a highly specialized augmentation technique is required. The subantral augmentation, clinically referred to as a maxillary sinus lift, is an established, highly successful, and heavily documented method to multiply vertical bone volume prior to insertion. The procedure involves accessing the maxillary sinus cavity, delicately elevating the Schneiderian membrane (the mucosal lining of the sinus) from the bony floor, and creating a new compartment. This surgically created void between the native jawbone and the elevated membrane is then densely packed with a selected grafting matrix, typically a slow-resorbing xenograft or a stabilized alloplast.
Historically, there were two primary approaches to this procedure: the direct (open) method and the indirect (closed) method. The direct method, often termed lateral antrostomy or the Caldwell-Luc operation, involves creating a bony window in the lateral wall of the maxilla to access the membrane directly. This approach is highly effective for massive volume augmentations but is considered more invasive. The indirect method, also known as the crestal approach or Summer’s technique, is a more conservative transalveolar approach where the sinus floor is accessed through the actual osteotomy site drilled for the implant, utilizing osteotomes and surgical mallets to fracture the sinus floor upward.
Regardless of the approach, the overriding challenge of the procedure is maintaining the absolute integrity of the Schneiderian membrane. This membrane is incredibly thin and fragile. A perforation or tear during elevation can allow the particulate graft material to spill into the sinus cavity, leading to acute infection, impaired mucociliary clearance, and the ultimate failure of the augmentation effort. Therefore, technological advancements over the past decade have focused entirely on minimizing trauma to this critical biological barrier.
The Physics and Application of Piezosurgery
Traditional surgical approaches, particularly the lateral window technique, relied heavily on high-speed rotary handpieces, diamond burs, surgical mallets, and chisels to cut through the maxillary cortical bone and access the sinus cavity. These conventional instruments carry a high inherent risk. A rotary bur spinning at tens of thousands of revolutions per minute cannot differentiate between hard bone and soft tissue. A momentary slip or excessive pressure can easily tear the delicate Schneiderian membrane or sever adjacent neurovascular bundles.
The introduction of piezosurgery has revolutionized the safety parameters of maxillofacial osteotomies. Piezosurgery is an advanced surgical technique for sectioning hard tissues while entirely sparing adjacent soft tissues, such as the brain, major nerves, and delicate mucosal membranes.
The technology operates on the precise physical principle of ultrasonic microvibrations. The piezoelectric device utilizes electrical energy to cause the expansion and contraction of piezoelectric crystals within the handpiece, generating specific ultrasonic frequencies. The device is meticulously calibrated to operate at a frequency typically between 25 and 30 kHz. This precise frequency bandwidth allows the specialized carbide tip to selectively cut highly mineralized hard tissues (bone). Crucially, soft tissues like the Schneiderian membrane or nerve sheaths require a significantly higher frequency—approximately 60 kHz—to be incised or damaged. Therefore, even if the vibrating ultrasonic tip comes into direct contact with the sinus membrane, the membrane vibrates along with the tip rather than being lacerated.
The mechanical action produces microvibrations of 60–210 mm amplitude with power exceeding 5 W, requiring very light handpiece pressure from the surgeon. Furthermore, piezosurgery utilizes an integrated saline coolant spray. This spray not only prevents thermal necrosis (overheating) of the surrounding bone but also creates a cavitation effect. The ultrasonic vibrations create microscopic bubbles in the saline that violently implode, creating a shockwave that helps to safely elevate the membrane hydrodynamically while clearing the surgical field of blood, vastly increasing visibility.
We use advanced techniques to minimize discomfort during a sinus lift dental procedure. The Piezoelectric Internal Sinus Elevation (PISE) technique exemplifies this advancement. In this technique, a specialized carbide tip with an indicating line for bone depth is used to prepare the osteotomy, replacing the traumatic surgical mallet and the hydraulic pressure historically used. Clinical studies heavily underscore this superiority. In massive cohort studies evaluating sinus lift procedures, researchers like Wallace et al. reported only 7 cases of Schneiderian membrane perforation out of 100 procedures using piezosurgery, while other researchers like Vercellotti et al. observed membrane perforations in a mere 5% of patients. This represents a monumental reduction in complication rates compared to the 20-30% perforation rates historically associated with rotary instruments. The precision of ultrasonic cuts combined with reduced surgical trauma translates directly to diminished postoperative edema, less reliance on analgesics, and a faster physiological recovery for the patient.
Osseodensification and Compaction Autografting
Beyond the implementation of piezoelectric technology for lateral approaches, contemporary transalveolar (crestal) sinus elevations frequently incorporate a paradigm-shifting concept known as osseodensification. Traditional implant site preparation relies on excavation—using fluted drills to carve and remove bone from the jaw to create a hole for the implant. In areas of soft, highly trabecular bone like the posterior maxilla, removing bone is counterproductive to achieving the necessary primary stability for the titanium fixture.
Osseodensification is a novel technique that reverses this methodology. Instead of excavating bone, this procedure utilizes specially designed high-speed densifying burs (Densah burs) that operate in a non-cutting, counterclockwise rotation. These hydro-pneumatic instruments feature a negative cutting angle and multiple flutes designed to preserve and compact the bone as the osteotomy is widened and the sinus floor is elevated.
The biophysics of this technique depend heavily on the viscoelastic nature of living bone tissue. In biomechanics, time-dependent stress produces time-dependent strain. By applying controlled, high-speed rotational pressure with copious irrigation, the bone plastically deforms rather than fracturing or cutting. The drills’ specific design promotes the compaction of the bone tissue laterally and apically into the surrounding trabeculae.
This creates an autografting effect. The bone that would normally be drilled out and discarded is instead compressed into the walls of the socket, drastically increasing the localized bone density. This heightened density dramatically improves the initial mechanical stability of the implant—the bone-to-implant contact (BIC)—which is a critical prerequisite for successful osseointegration, especially in immediate loading protocols.
Furthermore, as the bur advances apically, it safely lifts the cortical floor of the maxillary sinus without directly contacting or tearing the Schneiderian membrane, thereby minimizing the risk of perforation through a conservative, minimally invasive, and low-trauma procedure. Clinical studies comparing osseodensification to conventional PISE indicated that the osseodensification technique led to greater bone gain, improved bone density, shorter surgical durations, enhanced rapid healing, and significantly higher patient satisfaction metrics.
The Biological Power of the Schneiderian Membrane
Historically, the biological mechanisms driving bone regeneration within the enclosed space of an augmented sinus were subject to intense scientific debate. Early theories suggested that the bone growth emanated exclusively from the bony floor of the sinus cavity. However, recent groundbreaking clinical research has unequivocally proven the dominant, active role of the Schneiderian membrane itself.
In 2009, pivotal research by Srouji et al. redefined our understanding of sinus biology. They demonstrated that the basal cell layer of the Schneiderian membrane is, in fact, periosteum. Just like the periosteum that covers all vital bones in the human body, or the Dura mater covering the skull, this thin membrane is highly biologically active. It solely produces all necessary cellular and humoral factors required for bone healing and bone regeneration, most notably Bone Morphogenetic Protein 2 (BMP-2), which possesses a key function in initiating osteogenesis.
This vital periosteum alone can initiate bone regeneration and production even in the absence of any calcified structural graft material, provided there is a stable blood coagulum. When a grafting matrix is introduced, the membrane acts as the primary vascular and cellular source. Clinical observations using radiographic tracking noted that in procedures utilizing piezoelectric technology, an even and circular centripetal calcification under the sinus membrane and the antral floor could be detected. This calcification begins at the periphery (near the membrane) and moves inward toward the center of the graft. After four months, this newly mineralized tissue covers approximately 30% of the entire augmentation volume, and the calcification process is typically completed throughout the entire mass by the seventh month.
The results of these papers prove the key role of the sinus membrane as the main carrier of bone reformation after subantral procedures. Thus, the paramount importance of minimally invasive, rupture-free sinus lift procedures is scientifically underlined. If the membrane is torn, its osteogenic potential is severely compromised, highlighting why technologies like piezosurgery and osseodensification are not merely convenient tools, but essential instruments for biological success.
The Role of Platelet Concentrates and “Sticky Bone”
To further optimize the graft’s handling characteristics and maximize its biological potential, modern practitioners frequently utilize autologous blood concentrates. Despite years of effort, a solitary ‘perfect’ bone reconstruction material has not yet been developed in laboratories; therefore, a further effort is required to make this objective feasible by combining materials.
Platelet aggregates have been widely used to accelerate tissue regeneration and repair in various medical fields. In sinus floor augmentation, different bone grafting materials, alone or combined with concentrated growth factors, are used to achieve new bone formation as a prerequisite for fixture placement.
A highly effective clinical protocol involves the creation of “sticky bone.” Sticky bone is a fabricated, growth-factor-enriched bone graft matrix. It is created by drawing a small amount of the patient’s own blood prior to surgery and centrifuging it to isolate specific components. The surgeon then uses autologous fibrin-rich blocks combined either with Concentrated Growth Factors (CGF) or liquid Injectable Platelet-Rich Fibrin (I-PRF) matrices. When these concentrated, sticky fibrin networks are mixed with a particulate bone substitute (like a xenograft or alloplast), the resulting aggregate is highly stable and moldable.
This sticky bone matrix provides several immense clinical advantages. First, it physically holds the particulate graft together, preventing the migration of small granules into unwanted anatomical spaces or through small tears in the membrane. Second, the dense fibrin network resists micromovement during the critical early phases of healing. Third, and most importantly, CGF-CD34+ matrices are well known to actively accelerate new bone formation by releasing a slow, sustained dose of highly concentrated growth factors directly into the surgical site over several weeks. Case reports utilizing piezosurgical lateral approaches combined with tooth-derived bone grafts and CGF-CD34+ matrices demonstrated exceptionally good results in new bone formation after just 2 to 5 months, accompanied by a pain-free postoperative period devoid of complications.
The Histological Timeline of dental bone grafting recovery
The period following surgical augmentation is highly critical. The physical placement of the graft is merely the mechanical initiation of the therapy. The body must then execute a complex, highly orchestrated cascade of inflammatory, vascular, and regenerative responses to fully integrate the foreign matrix into the native skeletal architecture. Proper postoperative management dictates the success of this biological progression.
dental bone grafting recovery is not an immediate event; it is a meticulously orchestrated biological timeline that unfolds over several months.
-
Hemostasis and Clot Formation (Days 1-3): Immediately following the surgical intervention, the bleeding must cease, and a stable blood clot must form within the porous network of the graft and the surrounding surgical site. This coagulum is rich in platelets, fibrin, and essential growth factors. It serves as the initial biological glue, sealing the site and providing a provisional matrix for early cellular migration. The stability of this clot is paramount; if it is washed away or physically dislodged, the entire regenerative cascade fails, leading to localized osteitis (dry socket) or graft necrosis.
-
Inflammation and Angiogenesis (Weeks 1-3): A localized inflammatory response ensues. Macrophages infiltrate the site to clear microscopic cellular debris and any residual bacteria. Concurrently, the critical process of angiogenesis begins. Stimulated by the low oxygen tension in the center of the graft and the presence of growth factors, endothelial cells from the surrounding native bone proliferate and form new capillary networks that slowly infiltrate the grafted matrix. Without this rapidly developing vascular network, the deeper layers of the graft will remain avascular, necrotic, and incapable of supporting bone formation.
-
Osteoconduction and Osteogenesis (Months 1-4): As the blood supply is established, mesenchymal stem cells migrate along the newly formed blood vessels and attach securely to the micro-rough surface of the substitute material. Under the influence of BMPs, these cells differentiate into active osteoblasts. These osteoblasts begin secreting osteoid, an unmineralized, highly organic matrix composed primarily of Type I collagen. The osteoid is deposited directly onto the surface of the graft particles.
-
Remodeling and Maturation (Months 4-9): The secreted osteoid gradually mineralizes, incorporating calcium and phosphate to form hard, but structurally disorganized, woven bone. Over several subsequent months, this disorganized woven bone is systematically remodeled. Osteoclasts resorb the woven bone and any residual, resorbable graft material, while osteoblasts lay down mature, highly organized lamellar bone in its place. This lamellar bone is characterized by dense, parallel collagen fibers capable of withstanding the immense, multidirectional mechanical loads of daily mastication.
As previously noted, radiographic analyses of subantral augmentations reveal an even centripetal calcification under the sinus membrane that covers 30% of the augmentation volume by the fourth month, culminating in complete calcification by the seventh month. Interestingly, research also notes a slight volumetric contraction during this remodeling phase; a loss of approximately 13% of the absolute augmentation height is typically detected between the 4th and 7th month as the graft consolidates and matures.
Strict Postoperative Protocols for Graft Stabilization
To ensure the complex biological cascade proceeds uninterrupted from the initial hemostasis to final lamellar remodeling, patients must adhere strictly to a comprehensive postoperative care regimen. Failure to comply can easily disrupt the fragile angiogenesis phase, resulting in severe complications, including graft displacement, acute purulent infection, or complete failure of the augmentation.
A standardized, highly structured postoperative protocol is typically issued to patients following major grafting or sinus elevation procedures to ensure optimal healing and minimize complications :
-
Edema and Hematoma Management (Cold Therapy): Postoperative swelling is a normal physiological reaction to surgical trauma, typically peaking on the second or third day following the intervention. To actively mitigate excessive edema and prevent large hematoma formation, cold therapy is mandatory. Patients must apply ice packs to the affected cheek on the day of surgery and the following day, utilizing a strict interval protocol: 15 minutes of application followed by 30 minutes of rest. Direct pressure on the area must be avoided; the ice pack should be wrapped in a clean towel. The cold induces localized vasoconstriction, severely limiting the accumulation of fluid and blood in the interstitial facial tissues.
-
Mechanical Protection and Dietary Restrictions: The particulate matrix must remain absolutely stable for the delicate neovascular capillaries to form. Even microscopic micromovements can sever these newly formed blood vessels, halting bone formation. Consequently, a soft diet consisting entirely of room-temperature foods is strictly enforced on the day of surgery and must continue until suture removal. Hard, sticky, crunchy, or excessively hot foods must be completely avoided, as chewing forces could easily dislodge the graft material, disrupt the sutured incisions, or exert dangerous pressure on any simultaneously placed implants.
-
Sinus Pressure Mitigation and Sleeping Position: For patients who have undergone subantral augmentation, protecting the integrity of the Schneiderian membrane from drastic barometric pressure fluctuations is critical. Patients are instructed to avoid direct cheek contact with the pillow for the first two nights and to sleep with the head elevated using two pillows. This elevation utilizes gravity to reduce localized sinus congestion, prevent excessive venous blood pooling at the surgical site, and minimize facial swelling.
-
Barometric Precautions: Forceful alterations in nasal or sinus pressure can be catastrophic. Patients must absolutely avoid sneezing with a closed mouth; if sneezing is unavoidable, it must be done with the mouth wide open to vent the pressure. Forceful nose-blowing is strictly prohibited; if necessary, it must be done with extreme gentleness. Vigorous coughing should be suppressed or avoided for 2 to 4 weeks. Any sudden increase in sinus pressure from these actions could violently dislodge the sinus graft into the sinus cavity, cause a delayed membrane perforation, or force bacteria into the sterile surgical site. Minor postoperative bleeding from the nostril on the affected side is considered normal due to mucosal manipulation, but heavy bleeding requires immediate medical attention.
-
Infection Control and Oral Hygiene: The oral cavity is a highly contaminated environment colonized by billions of bacteria. Proper hygiene is absolutely critical for preventing surgical site infection, which could rapidly lead to purulent sinusitis or total graft necrosis. To keep the area clean, patients must rinse gently with a lukewarm saline solution (typically 3 times a day for 10 days). Aggressive swishing must be avoided. Patients must strictly avoid mechanical brushing near the sutured area while meticulously maintaining regular hygiene for the rest of the uncompromised dentition.
-
Physical Exertion Restrictions: Strenuous physical activities, lifting heavy objects, bending forward abruptly, or engaging in vigorous cardiovascular exercise must be paused until the sutures are removed and the initial healing phase is cleared by the surgeon. Increased cardiovascular output raises systemic blood pressure, which can easily induce delayed wound hemorrhaging, cause painful throbbing, or physically displace the carefully packed particulate matrix. Furthermore, patients are instructed to never manipulate, press, massage, or apply external pressure to the operated facial area to prevent any disruption to the graft stability.
The ultimate long-term success of the augmentation is heavily dependent on the biological quality of the selected xenograft materials and the patient’s strict, unwavering adherence to these precise biological parameters.
Economic Considerations and Global Dental Tourism
While the clinical necessity of bone grafting is indisputable for patients suffering from severe atrophy, the financial burden of these advanced procedures in Western healthcare systems is often prohibitive. In countries like Australia, the United States, and the United Kingdom, the cost of advanced piezoelectric sinus lifts, combined with premium biomaterials like BioOss or specialized low-temperature BCP alloplasts, can easily exceed the financial capacity of the average patient, especially since these procedures are rarely covered by standard medical insurance or public health schemes.
This economic reality has driven a massive surge in transnational dental care. Patients are actively seeking jurisdictions where the cost of living and operational overheads allow for significantly lower treatment fees without compromising the strict clinical protocols, biomaterial quality, or sterilization standards required for successful osseointegration.
When evaluating the cost of bone grafting, patients must consider the holistic value proposition. In premier international destinations like Vietnam, top-tier clinics employ internationally trained maxillofacial surgeons who utilize the exact same piezoelectric technology, Osseodensification Densah burs, and premium imported grafting materials as their Western counterparts. However, the comprehensive treatment packages are offered at a fraction of the domestic cost.
The most critical factor for patients seeking care abroad is verifying that the chosen facility adheres strictly to international infection control standards, such as those established by AAMI, and possesses the technological infrastructure (like 3D CBCT imaging and piezoelectric units) necessary to perform these complex subantral augmentations safely.
When executed with surgical precision, utilizing scientifically backed biomaterials, and respected deeply during the prolonged healing phase, the grafted site transforms from a structurally compromised defect into a rock-solid, biologically active foundation. This foundation ensures the lifelong mechanical stability and aesthetic success of the restorative fixture.
To receive a comprehensive evaluation of your alveolar bone density, contact our international patient support team for a specialized consultation.



Bài viết liên quan
Laser Teeth Whitening in Hanoi: Safe, Rapid & Bright Results
Achieve a brilliant, photo-ready smile with our professional teeth whitening hanoi services, completed in just...
Painless Teeth Scaling in Hanoi Old Quarter: Viet Bi Premium Experience
Disclaimer: This content is for informational purposes only and does not constitute professional medical advice....
How Long Do Implants Take? 7 Essential Timeline Facts
Patients frequently ask how long do implants take from the initial surgery to the final...
Dental Implant Materials Comparison: Titanium vs Zirconia
An objective dental implant materials comparison helps you choose the safest root replacement. You face...
Full Mouth Restoration in Vietnam: Options, Costs & Timeline
A complete full mouth restoration vietnam package includes advanced digital planning and premium materials to...
Teeth Implants for Seniors in Vietnam: Safe & Painless Solutions
Getting teeth implants for seniors requires specialized care and comprehensive bone density assessment. For older...